SECTION 10 STANDARD PROVISIONS FORMS
SP-10.01 Request for Information (SP-4.14)
SP-10.02 Substitution Request (SP-5.04)
SP-10.03 Subcontractor Statement of Acknowledgement (SP-8.01)
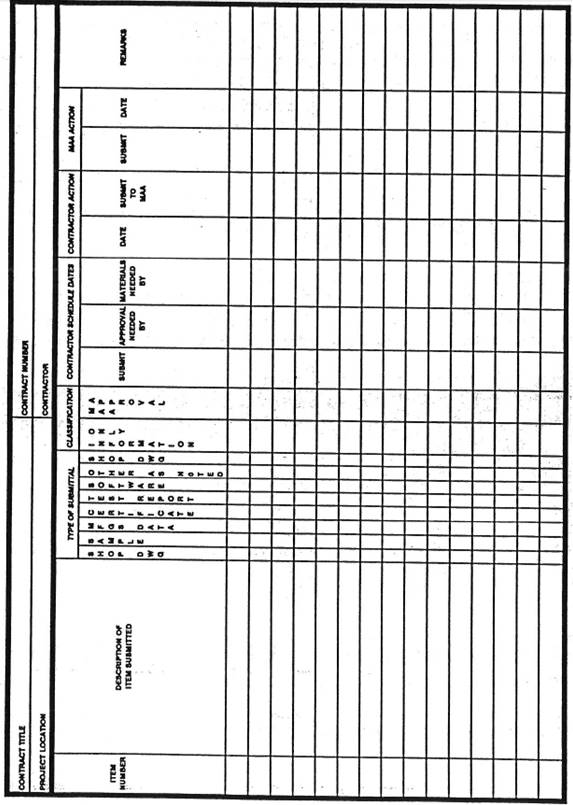
SP-10.04 Submittal Register (SP-8.06)
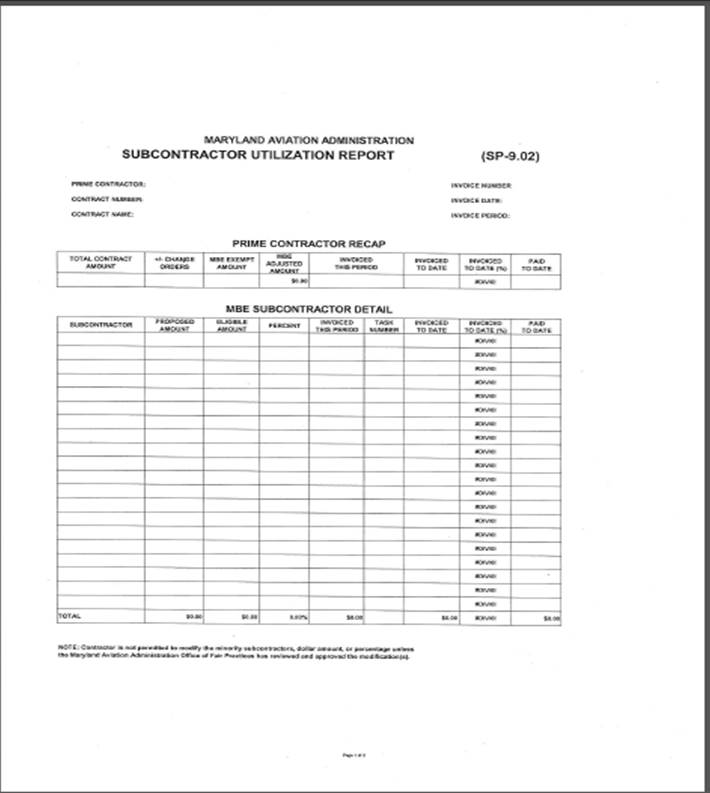
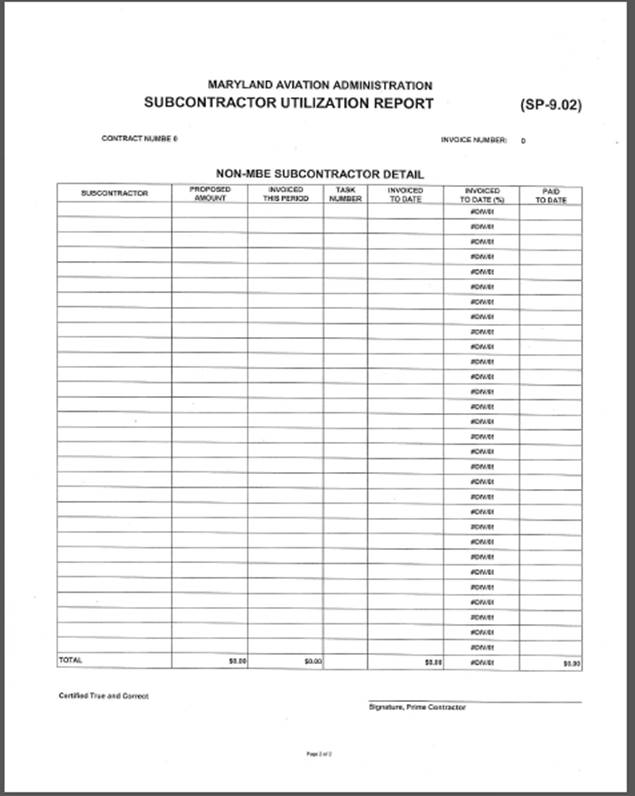
SP-10.05 Minority Business Enterprise Utilization Statement (SP-9.02)
SP-10.06 Monthly Injury Report (SP-6.04)
SP-10.07 Base Bid Schedule of Values (SP-2.02)
SP-10.08 Energized Equipment Work Permit (SP-4.17)
SP-10.01 Request for Information (SP-4.14)
|
Contractor: |
Contractor's Architect: |
||||
|
Address: |
Address:
|
||||
|
Phone: |
Phone: |
||||
|
Contract Title: |
Contract Number:
|
||||
|
RFI Number: |
Date of Request: |
Date Response Required (7 days minimum):
|
|||
|
Description of RFI:
|
|||||
|
As Built Sketches Enclosed: |
Specification Paragraph Ref: |
Drawing Reference:
|
|||
|
Contractor's Recommendation:
|
|||||
|
Cost Impact:
|
Schedule Impact: |
||||
|
Subcontractors Affected:
|
|||||
|
Subcontractors Coordinated With:
|
|||||
|
Submitted by: |
|||||
|
Architect/Engineer’s Response:
|
|||||
|
Response by: |
Date: |
||||
SP-10.02 Substitution Request (SP-5.04)
|
Contract Title: |
Item #: |
|
Contract Number: |
Section #: |
|
Contractor: |
Paragraph #: |
|
Item Specified: |
|
|
Proposed Substitution: |
|
Fill in the blanks below (incomplete forms will not be considered):
A. Does the substitution affect dimensions shown on the Drawings?
Yes No
B. Will the undersigned pay for changes to the building design, including engineering and
detailing cost caused by the requested substitution?
Yes No
C. What affect does substitution have on other trades?
D. What affect does substitution have on construction schedules?
E. Manufacturer's guarantees of proposed and specified items are:
Same Different
Explain if different:
F. Reason for Request:
G. Itemized comparison of specified item with the proposed substitution; list significant variations:
H. Accurate cost data comparing proposed substitution with product specified:
I. Designation of maintenance services and sources:
J. Attach complete technical data, including laboratory tests, If applicable.
K. Include complete information on changes to Drawings and/or Specifications which proposed
substitution will require for its proper installation.
L. Submit with the request all necessary samples and substantiating data to prove equal quality
and performance to the item specified in the Contract. Clearly mark the Manufacturer's
literature to indicate equality in performance.
|
The Contractor certifies that the proposed substituted product is of equal performance and assumes the liability for equal performance, design, and compatibility with adjacent materials.
The undersigned states that the function, appearance, and quality of the proposed substituted product is equivalent or superior to the specified item/product. Signature shall be the principal having the authority to legally bind his/her firm to the above terms. Failure to provide legally binding signature will result in retraction of approval.
Corporate Officer: _____________________________________________
Signature________________________________________________Date_____________
Address: ____________________________________________________
|
SP-10.03 Subcontractor Statement of Acknowledgement (SP-8.01)
|
PART I - STATEMENT OF PRIME CONTRACTOR |
|||||
|
1. PRIME CONTRACT #: |
2. CONTRACT TITLE: |
||||
|
3. SUBCONTRACTOR #: |
4. DATE SUBCONTRACT AWARDED: |
||||
|
4. PRIME CONTRACTOR (Name, Address, Phone)
|
5. SUBCONTRACTOR (Name, Address, and Phone)
|
||||
|
6.The Prime Contractor states that under the Contract shown in Item 1, a subcontract was awarded on the date shown in Item 4 by (name of awarding firm): to the subcontractor in Item 5 for the following work:
|
|||||
|
7. Name and Title |
8. Signature |
9. Date |
|||
|
PART II - ACKNOWLEDGEMENT OF SUBCONTRACTOR |
|||||
|
10.The subcontractor acknowledges that, as a minimum, the following clauses of the Contract shown in item 1 are included in the subcontract: |
|||||
|
GENERALSPECIALFEDERAL-AID CONTRACTOR AFFIRMITIVE PROVISIONSPROVISIONSPROVISIONSACTION PROGRAM |
|||||
|
GP-2.05SP-1.06FAA-1.04AAP-1.01 GP-7.01SP-6.03FAA-1.05AAP-2.02 GP-7.02SP-6.04FAA-1.06 GP-7.05SP-6.05FAA-1.07 GP-7.13SP-6.06FAA-2.06 GP-7.14SP-8:01FAA-2.12 GP-7.20SP-8.07FAA-4.02 GP-7.23SP-9.01FAA-4.03 GP-7.30FAA-4.05 GP-7.36 GP-8.01 GP-9.01 |
|||||
|
11. NAMES(S) OF ANY HIGHER, OR LOWER TIER SUBCONTRACTORS, IF ANY: |
|||||
|
12. Name and Title |
13. Signature |
14. Date |
|||
SP-10.04 Submittal Register (SP-8.06)
SP-10.05 Minority Business Enterprise Utilization Statement (SP-9.02)
|
Contract Title: |
Page _______ of _______ |
|
Contract Number: |
Date: |
|
Contractor Name: |
Invoice Number: |
|
MBE Utilization To-Date (%): |
MBE Goal (%): |
|
GENERAL CONTRACTOR STATEMENT |
||
|
Payment Through Last Period |
Payment This Period |
Total Payment To-Date |
|
|
|
|
|
MBE SUBCONTRACTOR PARTICIPATION |
||
|
Payment Through Last Period |
Payment This Period |
Total Payment To-Date |
|
MBE Subcontractor Number 1 (Name): |
||
|
|
|
|
|
MBE Subcontractor Number 2 (Name): |
||
|
|
|
|
|
MBE Subcontractor Number 3 (Name): |
||
|
|
|
|
|
MBE Subcontractor Number 4 (Name): |
||
|
|
|
|
|
MBE Subcontractor Number 5 (Name): |
||
|
|
|
|
|
MBE Subcontractor Number 6 (Name): |
||
|
|
|
|
|
MBE Subcontractor Number 7 (Name): |
||
|
|
|
|
SP-10.06 Monthly Injury Report (SP-6.04)
|
MONTHLY INJURY/ILLNESS REPORT (TO BE COMPLETED AND MAILED BY THE 7TH DAY OF EACH MONTH)
FOR THE MONTH OF: ________________________________________________
PROJECT NUMBER: PROJECT NAME: ___________________
PROJECT LOCATION: ________________________________________________
|
|
|
CONTRACTOR OR SUBCONTRACTOR NAME: _____________________________________________________________
ADDRESS:__________________________________________________________
|
|
|
TELEPHONE NO.: FAX NO.:
|
|
|
1. HOURS WORKED |
|
|
2. LOST TIME CASES |
|
|
3. RECORDABLE CASES |
|
|
4. LOST WORK DAYS |
|
|
5. CARRY OVER LOST WORK DAYS |
|
|
6. TOTAL LOST WORK DAYS |
|
|
COMMENTS:
|
|
|
PREPARED BY: DATE:
|
|
|
|
|
SP-10.07 BASE BID SCHEDULE OF VALUES (SP-2.02)
|
MARYLAND AVIATION ADMINISTRATION |
||||||
|
CONTRACT NO. MAA-C0-00-000 |
||||||
|
|
|
|
|
|
|
|
|
BASE BID SCHEDULE OF VALUES |
||||||
|
|
|
|
|
|
|
|
|
Division |
Item |
General Contractor |
Subcontractors |
Total Costs |
||
|
Labor |
Materials |
Labor |
Materials |
|||
|
|
|
|
|
|
|
|
|
Division 02 |
Site Work |
|
|
|
|
|
|
Division 03 |
Concrete |
|
|
|
|
|
|
Division 04 |
Masonry |
|
|
|
|
|
|
Division 05 |
Metals |
|
|
|
|
|
|
Division 06 |
Carpentry |
|
|
|
|
|
|
Division 07 |
Moisture Protection |
|
|
|
|
|
|
Division 08 |
Doors, Windows, Glass |
|
|
|
|
|
|
Division 09 |
Finishes |
|
|
|
|
|
|
Division 10 |
Miscellaneous Specialties |
|
|
|
|
|
|
Division 11 |
Equipment |
|
|
|
|
|
|
Division 12 |
Furnishings |
|
|
|
|
|
|
Division 13 |
Special Construction |
|
|
|
|
|
|
Division 14 |
Conveying Systems |
|
|
|
|
|
|
Division 15 |
Mechanical |
|
|
|
|
|
|
Division 16 |
Electrical |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Subtotal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GC General Conditions |
|
|
|
|
|
|
|
GC Overhead & Profit |
|
|
|
|
|
|
|
CQC Plan (Min. 3% of Subtotal) |
|
|
|
|
|
|
|
GC Mobilize / De-Mobilize |
|
|
|
|
|
|
|
GC Bonds |
|
|
|
|
|
|
|
GC Insurance |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Miscellaneous Allowance |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Totals |
|
|
|
|
|
SP-10.08 Energized Equipment Work Permit (SP-4.17)
MARYLAND DEPARTMENT OF TRANSPORTATION
MARYLAND AVIATION ADMINISTRATION
ENERGIZED EQUIPMENT WORK PERMIT
|
I. GENERAL INFORMATION |
|
|
Date |
|
|
Contractor Company Name |
|
|
Contract/Building Permit No. |
|
|
Contract/Building Permit Title |
|
|
Description of circuit/equipment |
|
|
Description of proposed work
|
|
|
II. TO BE COMPLETED BY CONTRACTOR |
|
1) Date and Time of Proposed Work
|
|
|
|
2) Location of Proposed Work (Attach exhibit of Floor Plan)
|
|
|
|
3) Detailed description of proposed work to be done including description of procedure to be used in performing work
|
|
|
|
4) Justification of why the circuit/equipment cannot be de-energized for the proposed work
|
|
|
|
5) Description of the safe work practices to be employed
|
|
|
|
6) Shock Risk Assessment |
|
a) Voltage to which personnel will be exposed: |
|
b) Limited approach boundary: |
|
c) Restricted approach boundary: |
|
d) Necessary shock, personal, and other protective equipment to safely perform work: |
|
|
|
7) Arc Flash Risk Assessment |
|
a) Available incident energy at the working distance or arc flash PPE category: |
|
b) Necessary arc flash personal and other protective equipment to safely perform work (If Arc flash label/ incident energy level label is not present, the contractor must take all necessary precautions for safety in accordance with the current applicable codes and standards): |
|
c) Arc flash boundary: |
|
|
|
8) Means employed to restrict the access of unqualified persons from work area
|
|
|
|
9) Name of Electrically Qualified Person performing proposed work
|
|
|
|
II.a. CONTRACTOR SIGNATURE |
|
|
|
Requestor’s Name and Title (Printed) |
|
|
|
Requestor’s Signature Date |
|
I have reviewed and agree that the above described work can be done safely.
|
|
Safety Manager Signature Date |
|
I. APPROVAL BY CMI REPRESENTATIVE |
|
|
|
Engineer’s Name and Company (Printed) |
|
|
|
Engineer’s Signature Date |
|
I. APPROVAL (FOR MAA USE ONLY) |
|
|
|
MAA Office of Facilities Maintenance Approver Name (Printed) |
|
|
|
MAA Office of Facilities Maintenance Approver Signature Date |